We are excited to announce that Brink is now part of Africa Practice. Learn more
When the rules break: Looking a gift horse in the mouth

Since U.S. President Donald Trump returned to office in January 2025, his administration has run roughshod over traditional multilateral institutions, turning development aid into a crucible, arguing it must be fundamentally reshaped. Out of the fire, the US has forged the new America First Global Health Strategy (AFGHS). The strategy is advertised as a replacement for traditional multilateral health assistance. It bypasses global institutions with bilateral health agreements that include commitments from recipient governments to increase their own domestic spending. The foreground for this new strategy has been Africa, with 22 of the 28 participating countries from the continent. The question many of them now face is whether the framework provides a sound foundation for a restructured partnership, or whether the retreat from development aid has simply given way to an artifice that may reveal something more sinister once African governments open their gates to it.
Growing independence or growing resource competition?
In attempting to raze the old global health architecture to the ground, the AFGHS taps into a long-standing anxiety about the previous system. That African governments’ reliance on external aid to fund their health system discouraged the development of domestic health systems by fostering dependency.
A key selling point of the AFGHS, therefore, is co-investment. According to the U.S. State Department, currently the AFGHS has paired USD 12.7 billion in US assistance with USD 7.8 billion in co-financing commitments from partner governments.
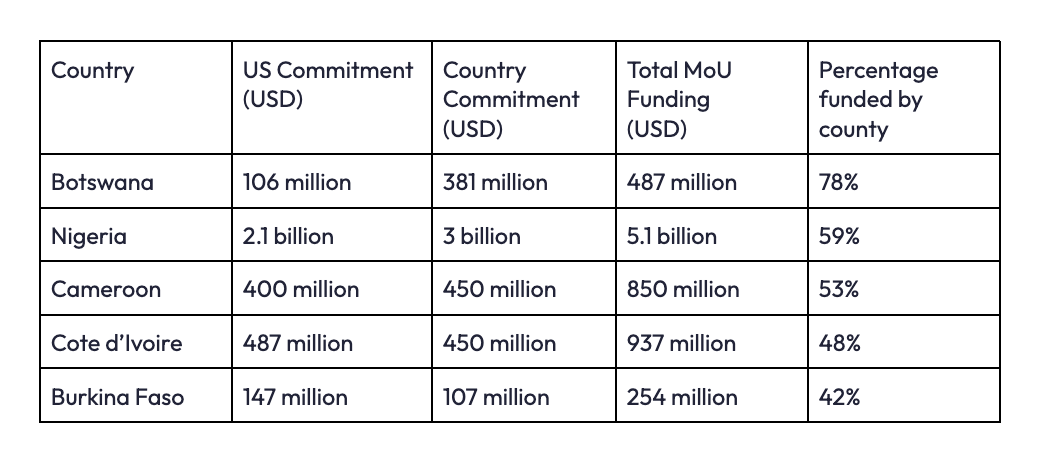
At first glance, this appears to speak directly to the dependency problem. Figure 1 highlights the MoUs with the largest percentage contribution from the recipient country, showing that this ranges as high as 78% in Botswana and 59% (USD 3 billion) in Nigeria. Securing domestic pledges for increased spending is not a new idea, however. In 2001, African Union states adopted the Abuja Declaration, pledging to allocate 15% of national budgets to health spending. Over the next 25 years, political commitment existed, but implementation capacity did not. By 2023, only two African countries had reached the 15% target, and research suggests that more than 90% of countries studied have less than a 1% probability of meeting the target by 2063. The new US agreements attempt to avoid this failure by tying funding to performance benchmarks and co-financing requirements. Yet they risk falling into the same structural implementation trap as Abuja, leaving governments chasing funding targets that they may struggle to meet, while giving Washington cover to withhold disbursements when they fail.
Nigeria, the country with the highest nominal commitment under the strategy, illustrates this well. Under its bilateral agreement, the expected additional annual co-financing requirement is approximately NGN 838 billion (USD 605.8 million), nearly 40% of Nigeria’s 2025 health budget allocation. To comply, Nigeria’s health budget would need to expand both significantly and rapidly. For a country whose health spending has historically been below 6% of the national budget, meeting this commitment appears highly unrealistic. The result may not be stronger, better-funded domestic health systems, but increased pressure to divert resources from other essential services, while accepting reduced US support, as Washington retains the discretion to scale back disbursements if commitments are not met.
American security first?
Another risk lies in how funding priorities are structured, with the US making little attempt to conceal the priorities underpinning its ‘America First’ strategy. While there is currently overlap between the US’ global health priorities and the priorities of African governments, there are signs of potential fissures.
The agreements are heavily oriented toward health security, particularly surveillance systems designed to detect infectious disease outbreaks before they spread internationally. From Washington’s perspective, this aligns with a national security imperative. However, the requirement for recipient governments to allocate funding toward these priorities may limit their ability to finance essential primary healthcare and other urgent health challenges that carry less risk of cross-border transmission, such as neglected tropical diseases and non-communicable diseases.
There is also uncertainty about the durability of US commitments themselves, given the overall position of the current US administration, including Robert F. Kennedy Jr., a prominent critic of vaccines. Under the AFGHS agreements, the United States retains the right to unilaterally pause or terminate funding if partner policies no longer align with US national interests.
While immunisation is a US priority in the current versions of these agreements, RFK-Jr sized agitations have already begun to ripple in the space. In February 2026, a USD 1.6 million trial funded by the U.S. Centers for Disease Control and Prevention (CDC) scheduled to take place in Guinea-Bissau, was cancelled by the host government over ethical concerns after the study plan proposed withholding the hepatitis B vaccine from infants. The trial was designed to examine broader claims about vaccine effects following questions raised by Kennedy. The incident not only raises broader questions about the future of vaccine funding commitments under an America First framework, but also about the political bias with which American-financed research in Africa will be conducted.
The signing of these agreements has also introduced a new layer of geopolitical conditionality, as access to negotiations increasingly appears linked to broader diplomatic alignment with Washington. South Africa, for instance, appears unlikely to see renewed bilateral HIV funding due to its sharply different positions from the United States on issues such as the Israel–Palestine conflict, US opposition to its domestic land expropriation policies, and wider diplomatic disagreements.
In other cases, the agreements function as both carrot and stick: the US agreement with Nigeria includes provisions directing approximately USD 200 million toward Christian faith-based healthcare providers, implicitly reflecting Washington’s concerns over the alleged persecution of Christians in the country. In Zambia, an AFGHS agreement was reportedly linked to negotiations over preferential access to critical minerals such as copper, cobalt, and lithium; a condition that ultimately contributed to Lusaka’s decision to reject the deal.
Devil is in the Datail
While the geopolitical dimension and Trump-era transactionalism have become increasingly explicit in the negotiation of these agreements, their content introduces another significant shift. Under draft guidelines circulated by the US government, which effectively represent Washington’s opening negotiating position, participating countries are to grant access to epidemiological data, genomic sequences, and biological pathogen samples.
While the financial commitments in many agreements extend for roughly five years, the data-sharing provisions are designed to last far longer. Proposed specimen-sharing arrangements could run for up to 25 years, while data-sharing obligations would remain in place for a decade after either party cancels the agreement.
The stakes are particularly high given that pharmaceutical companies and researchers rely on pathogen samples and genomic sequence data to design vaccines, diagnostics, and other medical countermeasures. Genomic data in particular allows for rapid vaccine and therapeutic development and enables commercial biomedical research, often without researchers needing direct access to the original samples. The COVID-19 pandemic illustrates the political and commercial implications of this system. African scientists shared viral genomic data early in the outbreak, yet many African countries waited more than 12 months after wealthier nations to achieve meaningful vaccine coverage. At the same time, estimates suggest that every dollar invested in COVID-19 vaccine development and delivery generated returns ranging from USD 42-775 globally.
Advancing fair and equitable benefit-sharing has long been a continental priority, predating the inequities exposed by COVID-19. In 2015, the African Union adopted guidelines on Access and Benefit Sharing to reinforce the principles of the Nagoya Protocol, which require countries’ consent before their biological resources are used and mandate agreed benefit-sharing. African states also supported the Pandemic Influenza Preparedness Framework, linking virus sharing to vaccine access. After these concerns came to fruition during the COVID-19 pandemic, African negotiators played a key role in advancing a Pathogen Access and Benefit-Sharing (PABS) system under the 2025 WHO Pandemic Agreement, aimed at guaranteeing developing countries access to vaccines and technologies derived from the pathogen data they provide.
All these collective efforts to embed equity now risk being sidestepped by the new agreements. The United States withdrew from PABS negotiations before leaving the World Health Organization in January 2026, while concerns over data sovereignty have become a central point of contention in the bilateral deals Washington is advancing. These concerns have prompted some governments to reject the agreements and sparked criticism from stakeholders even where governments have signed them. Both Zimbabwe and Zambia rejected proposed deals, with Zimbabwe citing the lack of guarantees on benefit-sharing from future vaccines and treatments. In Kenya, the government secured amendments to align data-sharing provisions with Kenyan law, but stakeholders have since challenged the agreement in the Supreme Court, which is reviewing its legality.
Ultimately, these agreements risk bringing the system close to where it began, except that instead of negotiating collectively through multilateral frameworks, countries are now approached individually. Most importantly, by accepting terms with fewer safeguards around equitable benefit-sharing, countries such as Nigeria may inadvertently reinforce long-term dependency within their domestic pharmaceutical sectors. Without provisions for technology transfer or shared intellectual property, the value of the data provided by these countries can be absorbed by multinational firms, leaving local industries reliant on importing the resulting products rather than building the capabilities to produce them themselves.
Holding the line together
While resistance is beginning to emerge, the central logic of the AFGHS is to weaken collective bargaining by engaging countries individually. Ultimately, this reflects a broader shift in the rules of global politics. Multilateralism and globalisation once promised mutual restraint, with interdependence acting as a brake on reckless behaviour because states depended on shared systems. Increasingly, that same interdependence is being inverted into a source of strategic leverage and a locus for transactionalism.
In response to shrinking aid flows, the African Union has argued that the path out of dependency does not lie simply in attracting more external funding, but in addressing inefficiencies within existing health systems. Its analysis suggests that African health systems operate at roughly 77% efficiency, meaning that around 23% of health spending is lost through misallocation, fragmentation and administrative leakage. Therefore, in a world where the rules are breaking down, the response is either to hold the line collectively or rethink the rules together. I would argue, as the AU does, that the route out of dependency will not be found by “chasing more money, but by stopping the massive inefficiencies and waste in the money already available.”



Proud to be BCorp. We are part of the global movement for an inclusive, equitable, and regenerative economic system. Learn more